
If you prefer that healthcare be proactive rather than reactive, population health management might be for you.
In 2000s, the term population health was relatively new in America, though it had been in use in Canada and the U.K. since at least the 1990s. In a 2003 article published to the American Journal of Public Health, What is Population Health, authors David Kindig and Greg Stoddart defined the term.
“We propose that population health as a concept of health be defined as ‘the health outcomes of a group of individuals, including the distribution of such outcomes within the group.’ These groups are often geographic regions, such as nations or communities, but they can also be other groups, such as employees, ethnic groups, disabled persons, or prisoners.”
The concept of population health has since become an accepted part of healthcare, and one that is a prominent driver of the value-based healthcare system. After all, if value-based healthcare is to be successful, examining elements affecting the efficacy of that care (including population-based factors such as location, social status, age and ethnicity) should be part of the process.
Population health management, consequently, has grown into an increasingly influential element in the healthcare industry over the last 10 years.
What Is Population Health Management?
Population health management (PHM), a fundamental part of managed care, is a discipline focused on Improving population health, enhancing patient experience, and reducing per capita cost — known in healthcare as the Triple Aim.
In 2008, the Institute for Healthcare Improvement (IHI) developed the three-part approach referred to as Triple Aim. Healthcare leaders and policy makers have widely accepted the approach during the gradual transition to value-based care.
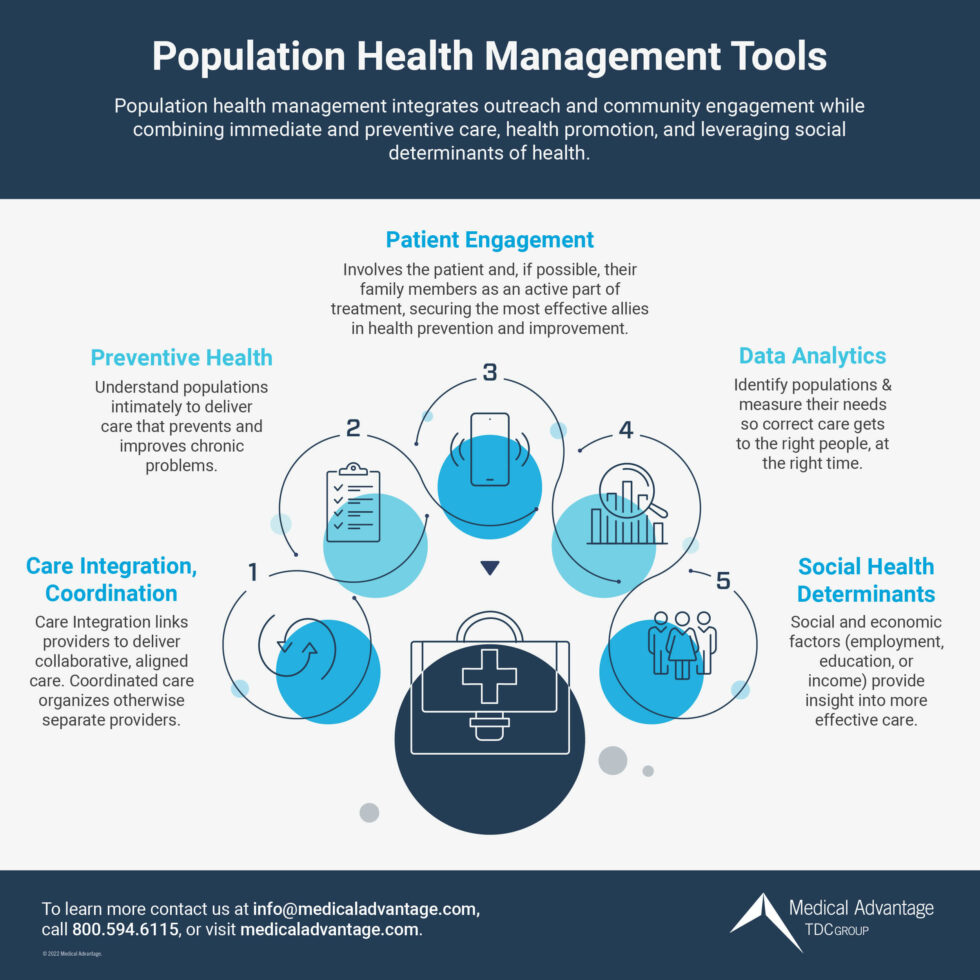
The discipline integrates active outreach and community engagement while combining immediate and preventive care, health promotion, and active application of social determinants of health.
Dr. J. Collins Corder defines population health management in a Missouri Medicine Journal article. In the piece, he calls PHM, “the aggregation of patient data across multiple health information technology resources, the analysis of that data into a single, actionable patient record, and the actions through which care providers can improve both clinical and financial outcomes. The goal is to improve the health outcomes of the group by monitoring and identifying individual patients within that group, using a business intelligence tool to aggregate data and provide a comprehensive clinical picture of each patient.”
PHM as a discipline holds much potential to improve health outcomes and control costs, since, as Corder says, about 80 percent of what affects health outcomes falls outside the traditional boundaries of healthcare delivery. Those factors that are all generally common knowledge, but are seldom assessed as a whole, include:
- Health behaviors (such as tobacco use, or sexual activity)
- Social and economic factors (employment, education, or income)
- Physical environment (air quality or water quality)
The idea became very popular, so much so that Google trends show searches for the term “population health management” rising nearly 4-fold from 2009 to 2015, Dr. Ashish K. Jha wrote in the JAMA forum.
Key Components of Population Health Management
The key components of population health management are:
- Care integration and coordination
- Patient engagement
- Data analytics
- Preventive health
Affecting all these components are:
- The social environment (income, education, employment, social support, culture)
- The physical environment (urban design, clean air and water)
- Genetics
- Individual behavior
The four key components of population health in more detail:
Care integration and coordination
An integrated delivery system (IDS)manages and improves clinical outcomes and is a collaborative network linking providers to provide healthcare for a specific population. This element coordinates care among separate providers, ensuring the care provided is a cooperative effort working off the input of each specialist treating a patient for a particular problem. Accountable Care Organizations (ACOs) incorporate this practice by improving coordination and communication among health professionals treating with the same patient. They bring together healthcare delivery elements: primary care, specialists, hospitals, and home health, ensuring they are all working together.
Patient engagement
Patient engagement involves the patient and, if possible, their family members as an active part of the team working to solve problems. By having the patient and those closest to the patient actively participating in the care plan, you will have secured your most important allies in improving health outcomes. Patients and families motivated to engage in patient care often become active partners in care planning, improving the chances that health outcomes are achieved.
Data analytics and Health Information Technology (HIT)
Data is useful for identifying populations and measuring their needs so that the correct care will be provided to the right people, at the right time.
Data analytics can track key performance indicators (KPIs) including patients by day, by age group, by specialty needed, and total patients, providing insight into who your patients are, and their needs, so practice staff and services can be tailored to respond appropriately.
The tools can also be used to monitor the overall health of specific populations, pointing out, for instance, a town where substance use is a developing problem, or where empty nesters are aging into situations requiring more medical services. Data on patients’ living conditions, history of falls, transportation availability and medications can all be used to better predict the type of care or intervention that may prevent the number of fall injuries such as broken bones and hips.
Analytics can also be used to ensure that preventive medicine (such as colorectal screenings, breast cancer screenings and cervical cancer screenings) is applied at the right time.
Preventive health
Speaking of screenings, preventive efforts lie at the heart of population health. Population health seeks to understand populations intimately to deliver the proper care as needed, certainly. The old adage, “an ounce of prevention is worth a pound of cure” applies, as behaviors and habits have the power to damage a patients’ health that often cannot be undone.
Where population health truly shines, however, is in providing the guidance to better time and deliver that preventative healthcare. As many undiagnosed diabetes patients will tell you, you need to know there’s a problem if you hope to do anything about it.
Goals of Population Health Management
Population Health Management goals include improving health conditions of current patients while understanding the needs of future patients who may have been overlooked and improving overall healthcare at the population level. People are social. Sometimes the best way to improve a single person’s health is by informing the behaviors of the groups they belong to.
The goals of Population Health Management, in fact, align with the goals of Accountable Care Organizations, according to NCQA’s Population Health Management Resource Guide. The primary objective of ACOs is to organize providers to deliver coordinated, high-quality care in order to spend healthcare dollars wisely.
The overall goals of population health management (mentioned earlier as elements of the Triple Aim) fall under three categories: improving population health, making patient experience better, and reducing cost. NCQA distills that further, “The goal of PHM is to maintain or improve the physical and psychosocial well-being of individuals and address health disparities through cost-effective and tailored health solutions.”
Why Is Population Health Important to Value-Based Care
Federal, and, in some cases, state, policy has driven a focus on population health management and value-based care in recent years.
For example, there was Massachusetts’ healthcare reform led by then Republican Governor Mitt Romney, later coined “Romneycare”. Its later derivative federal cousin was the Affordable Care Act led by President Barack Obama (also known as “Obamacare”). “Obamacare” was, in fact, modeled after “Romneycare”. The two sets of legislative reform share many elements that seek to limit costs while improving care, often as a result of improving care.
Value-based care applies population health to identify patient risk, target interventions, and monitor progress.
“Development of a comprehensive population health management strategy is critical to an organization’s ability to drive outcome improvements and succeed under value-based payment models. Organizations must be able to identify the needs of their populations through assessment, risk stratification and development of programs and services that are tailored to those needs,” NCQA notes in its white paper,
Reducing Costs with Value-Based Care
Value-based care produces outcomes that are the best of both worlds. It applies data-proven approaches to target the correct care where it will be most effective while avoiding wasteful, ineffective treatment and services.
Better healthcare is not just better for patients – it is also less costly in the short term as unnecessary and ineffective care is wrung out of the system. It is also cheaper in the long run, According to NCQA’s white paper. “Population health gained further national attention when Donald Berwick and colleagues at the Institute for Healthcare Improvement included, ‘improving the health of populations’ as one of the three elements of the Triple Aim. The Centers for Medicare & Medicaid Services (CMS), under Berwick’s leadership, later adopted the Triple Aim as a strategy to focus policymakers’ attention on the simultaneous pursuit of improving the patient experience of care, improving the health of populations and reducing the per capita cost of healthcare.”
Value-based care reimbursement requires effective population health management that improves a patient’s experience and quality of care, lowers healthcare costs and improves outcomes. Population health management helps maintain and improve the physical and mental well-being of individuals, addressing health disparities through cost-effective, customized healthcare.
Why Looking at Population Data Can Help Value-Based Care Goals
Value-based care models reward practices that reduce their use of expensive, redundant or low-quality care. The surest way to assess and avoid those is with population data and analytics.
Population Health Management is a data-driven endeavor, and that data can produce very effective results. NCQA’s white paper provides the example of the Medical Home Network (MHN), in Illinois, which reduced the total cost of care trend for 170,000 people by 3.5 percent in year one and by five percent in year two by launching a value-based model in an integrated delivery system of more than 300 entities. MHN did that by achieving an 82 percent completion rate for health assessments, compared to rates well below 50 percent for comparable organizations.
To understand the risks and needs of the population, MHN integrated health assessment results with data from other sources, including claims data and admission and discharge data. “This allowed MHN to focus its population health management strategy and apply prioritized, real-time alerts sent to delegated care managers at the practice level,” NCQA reported.
Developing Population Health Management Strategies for your Practice
Improving population health through population health management requires developing a plan and strategy.
The population health management strategies you decide upon will be as unique as the healthcare goals you strive toward, and populations you work with. Data analytics will provide the clues you will need to develop the strategy needed to achieve your goal. Clues to strategies to improve care may come from socioeconomic, environmental, genetic, behavioral or geographic factors, which all affect patient health.
Population health management strategies are not only specific to their populations, they’re also dynamic – specific to and applicable to the time in which the data was analyzed. A strategy decided upon at one time, even with the same population, may need to be adjusted over time, since all these factors are in flux.
Upgrade Your Data Analytics to Better Understand Population Health
The ability to see population health data with analytics and dashboards is, therefore, integral to understanding where your practice stands and how best to meet your goals from that point. Dashboards that present population health data in easily adjusted formats will be key to making quick, informed decisions.
Creating Plans to Better Serve the Underserved
Population health analytics and dashboards will also help you develop plans to better serve your underserved patients. With the right guidance, you will be able to meet patients where they are with telehealth solutions. Depending on what the data says about your patient populations, additional methods to increase access to care may be uncovered.
Improve Outreach to Properly Identified Patients
Once you have the data that shows who your patients are, where they are, what their needs are, and when it is needed, you can create an outreach plan to ensure patients’ needs are met.
Medical Advantage Can Help
Medical Advantage offers patient, patient visits, and services healthcare dashboards designed to give your organization the insight necessary to make sound strategic decisions, improve care quality, and boost revenue. In addition, our dashboards provide not only insights into your data, but a bridge to our expert consultants – who can advise on and implement changes based on findings in your data. We also offer a wide range of services to alleviate the burden of implementing value-based care. Starting with EHR optimization, our consultants can assist your practice in documenting care efficiently and accurately, ultimately improving VBC performance.



